Khalaf Mohamed Khalaf Almazrouei1*, Reham Kotb2,3, Ohod Abdulla Salem4, Asmae Mohammed Oussaid5, and Aisha Mohammed Al-Awlaqi6, Heba Mamdouh7
1*Abu Dhabi University, COHS Public Health Muhawi, Abu Dhabi, UAE, [email protected], ORIC ID: 0009-0005-3157-1409
2Abu Dhabi University, College of Health Sciences, Abu Dhabi, UAE, [email protected], ORIC ID: 0000- 0003-1783-4370
3Alexandria University, Egypt, High Institute of Public Health, Department of Primary Health Care
4Abu Dhabi University, Abu Dhabi, UAE, [email protected], ORIC ID: 0009-0002-0167-6224 5Abu Dhabi University, Abu Dhabi, UAE, [email protected], ORIC ID: 0009-0006-6949-2252 6Abu Dhabi University, Abu Dhabi, UAE, [email protected], ORIC ID: 0009-0001-3300-2294
7Alexandria University, Egypt, High Institute of Public Health, Department of Family Health, [email protected], ORIC ID: 0000-0002-7273-915X
Abstract
Introduction: Premarital screening and counselling are essential diagnostic programs which aim to reveal genetic conditions infectious diseases and non-infectious long-lasting illnesses in couples before marriage.
Objectives: This research aims to evaluate the knowledge, attitude, and practice (KAP) levels among a sample of university students who live in Abu Dhabi, United Arab Emirates (UAE), regarding premarital screening and consultations.
Methods: The study had adapted cross-sectional approach conducted between September 2022 and January 2023 before premarital genetic testing became mandatory in the UAE on January 25, 2025 during which 380 participants from university were recruited through snowball sampling methodology. An online questionnaire containing premarital screening and consultation-related questions had been developed to collect data for KAP evaluation from study participants.
Results: Results demonstrate that 70% of survey participants know about premarital screening since 8% obtained their information through family members and healthcare workers, and friends. The knowledge of particular hereditary diseases alongside screening benefits remains incomplete among population segments. The results revealed the participants’ approval for an obligatory premarital screening initiative containing mental health evaluations since more than 75% of the participants supported this program.
Conclusion: The research findings present essential reasons to enhance premarital screening education delivery, focusing on extending knowledge about tests at baseline for better patient compliance.
Keywords: Premarital Screening, Knowledge and Attitude, Practice for Hereditary Diseases, Abu Dhabi, UAE.
© The Author(s) 2025. Open Access This article is licensed under a Creative Commons Attribution-NonCommercial- NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third-party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Introduction
Studies show marriage functions as a social tool for nations to create enduring family connections between generations [1]. The United Arab Emirates (UAE) preserves marriage as its core cultural tradition but the legal structure derives from Islamic law through its traditional social customs [2]. Laws based on social traditions have led public agencies to face increased pressure for testing all prospective couples before marriage. The combination of contemporary disease-prevention methods applied to genetic conditions caused through consanguineous relationships has modified these population statistics. Both the marriage stability and the health of the fetus require the essential pre-marital medical screening process for disease detection [3]. The UAE government implemented premarital screening to combat increasing genetic disorder risks because of traditional consanguineous marriage traditions throughout the Gulf region [4]. The data shows that consanguineous relationships form 50.5% of all Emirati marriages and create a higher possibility for recessive diseases like sickle cell anaemia and thalassemia and cystic fibrosis and others [5, 6]. Premarital healthcare services received crucial improvements from the UAE to combat public health threats. The UAE Ministry of Health and Prevention introduced genetic tests in all Emirati premarital screenings that began in January 2025. The complete test panel includes 570 genes that detect 840 known medical conditions, thus helping to identify serious genetic diseases early [7]. The initiative aims to decrease genetic disease load by improving reproductive healthcare education alongside professional medical counselling for prospective couples. Multiple studies have confirmed the advantages of premarital screening practices. The practice of premarital screening assists couples in preventing serious genetic and infectious diseases from spreading between them and helps create better pregnancy outcomes with better preparation for long-term health [8]. The UAE’s mandatory premarital screening program finds public interest lower among younger generations despite its clear advantages. The continuous inhibition of complete premarital service usage develops from a mix of concerns regarding social judgment, result interpretation errors, confidentiality doubts, religious beliefs and minimal health literacy understanding [9, 10]. The student population appearing at universities has critical importance for studies that evaluate understanding along with behavioural aspects regarding premarital screening procedures [11]. The young adults who are about to start their marital life will determine the program’s success in the coming years because of their current decisions and actions. Premarital screening perceptions of these young adults develop through public health education guidelines and their interaction with peers and family members, along with their religious beliefs and personal convictions. Public health information interacts with cultural peer and family experiences and religious principles, and personal preferences to shape students’ opinions about premarital screening [12, 13].
Research based in the UAE alongside neighbouring Gulf nations has investigated public opinions on premarital testing to produce vital findings [9, 14]. The research conducted by Al- Farsi et al. [15] discovered that most participants endorsed premarital testing however, they maintained misconceptions about the prevention abilities of screening, combined with a poor understanding of what happens following positive results for diseases. Studies conducted with medical students in Saudi Arabia and Qatar demonstrated that students of scientific disciplines exhibit cultural and emotional concerns regarding how testing results will impact their marriage prospects [9, 10]. The perception and interaction patterns of university students regarding premarital health services in Abu Dhabi lack modern data investigation, particularly since recent policy developments [16]. Future National Genetic Disease Prevention Program interventions in the UAE need comprehensive knowledge of youth deficits and factors that shape their preventive behaviours against genetic diseases. Thus, this study has been conducted to determine the knowledge, attitudes, and practices of university students in Abu Dhabi, UAE, regarding premarital screening and consultations. This study utilizes a cross-sectional survey that investigates both the level of understanding among participants and their misconceptions, as well as their screening readiness and their perceived obstacles to their involvement. The gathered research data will produce crucial findings which answer how young adults respond to current public health initiatives, as well as recognize methods to increase community-level health management commitment and disease prevention knowledge.
Materials and Methods Study Design and Setting
This study employed a cross-sectional descriptive approach to measure the knowledge, attitudes, and practices (KAP) of premarital screening and consultations among Abu Dhabi university students in the United Arab Emirates (UAE). The research took place in Abu Dhabi City, where a university enabled researchers to access students from various demographics who fell within standard marital age parameters. This study was conducted between September 2022 and January 2023 before premarital genetic testing became mandatory in the UAE on January 25, 2025, assessing university students’ knowledge, attitudes, and perceptions of screening to inform future public health policies. Research data generated in real-time allowed policy makers to build health education strategies which facilitated outreach activities throughout the UAE.
Study Population and Sampling Technique
This study evaluated university students from 18 to 60 years old who contributed to the research sample within Emirati and wider expatriate communities in Abu Dhabi. To gather insights regarding marital life the research study recruited single and married male and female university students. The research utilized non-probability snowball sampling to recruit participants during its study [17]. The non-probability snowball sampling began its participant selection process through student contacts at the university with additional referrals made through digital channels. The study participants who accepted research participation invited their online connectivity peers to recommend participants. Researcher chose this technique because random sampling methods failed to work effectively while exploring culturally sensitive premarital topics. The non-random method enabled researchers to establish a bigger pool of willing participants while protecting sensitive confidentiality requirements at the same time [18].
Sample Size Determination
The Centres for Disease Control and Prevention (CDC) produced the EPI Info version 6.0 software which determined our minimum adequate sample size. Researchers applied these exact criteria to run the sample size calculation. Our data collection used a 5% margin of error for 95% confidence and 90% statistical power. A standard method of 50% expected proportion determination for primary variables in unknown prevalence situations generates largest needed sample sizes. The software program determined that our study needed 380 participants based on the information we provided. We implemented this number to account for incomplete responses and sample dropouts while maintaining sufficient power for analyzing the final research sample data. Prior to analysis, the dataset was screened for incomplete responses. Surveys with more than 20% missing data were excluded from the final analysis. For isolated missing values, listwise deletion was applied. The final analytic sample consisted of 380 fully completed surveys, ensuring adequate power based on the original sample size calculation.
Data Collection Tool and Procedure
The researchers employed an online version of their structured self-administered questionnaire distributed in English to collect data. The research team created the questionnaire by examining relevant studies and using established existing assessment instruments for premarital testing and health practices. It consisted of 27 questions divided across four main sections, including socio-demographic factors, premarital screening knowledge, screening attitudes, consultation preferences and actual or planned screening procedures. The survey adopted both open-ended and closed-ended formats, which allowed for a combination of free-response and standardized answers. The research study included an ethical contact point for participants to enter their information to ask questions about the study procedures. Before proceeding with the survey, participants needed to read and electronically confirm the consent form that appeared at the beginning of the questionnaire. The questionnaire underwent a validation process. A pilot study was conducted involving 30 university students from the same institution [19]. Feedback obtained led to minor revisions in language and item structure to enhance clarity, cultural relevance, and respondent comprehension. The initial testing phase produced results that led researchers to change numerous statements to create questions which are direct and culturally appropriate. The pilot phase participants were removed from the final data collection to ensure unique research outcomes and comply with research standards.
Variables and Measurement
The survey collected essential demographic data points that included respondent age along with gender identity and nationality (Emirati or non-Emirati), marital status (single, married, separated and divorced or widowed), education level (high school/diploma, bachelor’s degree or post-graduation), employment status (employed or unemployed) and estimated monthly income categories (less than AED 5,000 or between AED 5,000 and AED 20,000 and above AED 20,000). The survey presented knowledge-based screening questions about premarital screening requirements in the UAE, and participants demonstrated their understanding by showing awareness from different information sources about the procedure and its legal requirements. The survey asked participants about their understanding of how avoiding screening tests affects future relationship prospects and their understanding of required screenings for handling romantic and social relationship issues that married individuals encounter.
The survey evaluated attitudes regarding mandatory screenings and mental health screening integration, together with preferred actions following contradictory results in premarital genetic testing. The options for responding to incompatible screening results included proceeding with genetic counselling or delaying the wedding, pursuing extra tests or refusing to have children. Participants answered questions about their past pre-marital screening experiences, as well as their plans to recommend screening and their familiarity with unscreened marriages.
Statistical Analysis
The Statistical Package for the Social Sciences (SPSS) version 29.0 served as the tool for analyzing all gathered data [20]. Analysis for demographic characteristics alongside the knowledge and practice, and attitude responses used descriptive statistical methods. The chi- square tests identified statistical significance when p-values remained under 0.05 for variable associations. A breakdown of categorical data was presented using frequency tables, and the percentage of cases was calculated. A p-value lower than 0.05 revealed statistical significance as measured by chi-square tests to confirm key variable relationships. A rigorous system protected the confidential data. The data statistical processes and visual representations were conducted through RStudio version 2023.03.o and Microsoft Excel 2020 for accuracy and presentation improvement.
Ethical Considerations
The Institutional Review Board (IRB) at Abu Dhabi University approved research ethics during this study. Every participant joined the study voluntarily and received notification about their right to exit at any moment with no requirement to state a reason. The questionnaire began after participants provided their electronic consent. Research data protection guidelines served as guidance for the entire investigation procedure. The data collection procedure included full anonymity, and the data was encrypted and password-protected in a device which only the principal investigator and authorized co-investigators could access. The system contained an automated data deletion protocol which triggered data deletion during unauthorized access attempts to maintain complete confidentiality.
Results
Table 1 presents the demographic composition of research participants based on sociological characteristics. Most participants (71.8%) were between 18-28 years old, and females dominated the sample population (73.7%). The survey included almost equal proportions of UAE national participants at 47.1% and non-UAE nationals at 52.9%. Non-married individuals constituted the largest group at 67.4%, followed by 23.2% married couples, and 2.9% were divorced individuals. The educational attainment of participants revealed that bachelor’s degree holders made up 48.9% of the sample, and high school graduates and diploma holders combined for 36.1%. Data showed that 58.4% of participants remained unemployed, yet 46.3% earned less than 5,000 AED per month, while 18.2% exceeded 20,000 AED per month.
Knowledge of Pre-Marital Screenings and Counselling
The Table 2 data summarizes the initial sources participants used to obtain information about premarital screening services and rules of counselling. Interestingly, large proportions of respondents (70.8%) were to some extent aware of these services, mainly through their owns networks (31.1%), health providers (22.1%), and the media (15.8%). However, premarital screening was an experience used by only 36.3% of participants prior to their marriage. Regarding the awareness of the diseases, HIV was reported as a disease frequently included in the premarital screening by 56.3% of respondents, followed by thalassemia (51%) and hepatitis B (48.2%). Knowledge of such ailments as G6PD deficiency and syphilis was much lower (20.0% and 27.4%, respectively). Notably, 14.5% of the respondents had no idea of any particular diseases that were being tested during such screenings. Most of the respondents (85.8%) were in agreement that premarital testing might aid in preventing the transmission of genetic disorders, and 86.1% would require these tests to be mandatory among UAE nationals. Moreover, 83% believed that marital satisfaction might suffer in the absence of screening. Interestingly, 62.4% had personal acquaintance with couples who had married without such tests. Lastly, 85.8% obtained a notion that premarital screening contributes to circumventing future psychological and social difficulties in families.
Attitudes and Practices Regarding Pre-Marital Screenings
The table 3 contains information that demonstrates the attitudes of the participants concerning premarital screenings and counselling. A considerable number (82.7%) agreed to add mental health tests to the screening. In the event of possible incompatibility indicated by testing, 64.5% said they would rethink their decision to get married. Interestingly, an equal percentage also indicated that they would have married had the screening outcome been positive, showing ambivalence with regard to health outcomes. The percentage of partners who obeyed genetic counselling or therapy as an option to investigate any reproductive possibilities was 37.8% in a scenario where, both partners were found carrying genetic disorders. Conversely, only 22.8% were willing to forfeit the marriage. A tiny percentage thought about alternatives (adoption 2% or not having children 9%). Furthermore, 11.5% would consult a professional, whereas 16.9% would want to see more information to gain a better insight into the toll of such a situation on them.
Table 3: Participants’ attitudes and practices regarding pre-marital screenings and counselling
| Item | Frequency (N) | Percentage (%) |
| Ever undergone premarital screening | ||
| Yes | 138 | 36.3% |
| No | 115 | 30.3% |
| I am not married | 127 | 33.4% |
| Steps for couples who are carriers of a disease | ||
| Therapy/genetic counselling | 151 | 39.8% |
| Call off the wedding | 87 | 22.8% |
| Seek assistance | 44 | 11.5% |
| Want more information and tests | 64 | 16.9% |
| Adoption or not having children | 34 | 9.0% |
| Agree that mental health should be included | ||
| Yes | 314 | 82.7% |
| No | 24 | 6.3% |
| I don’t know | 42 | 11.1% |
| Willing to reconsider marriage decision | ||
| Yes | 245 | 64.5% |
| No | 135 | 35.5% |
| Will advise future spouse to do premarital screening | ||
| Yes | 265 | 66.7% |
| No | 115 | 30.3% |
Barriers to Pre-Marital Screening and the Need for Education
Figure 1 indicates the most significant factors that hinder the process of couple take up of premarital screening tests. Citing financial constraints, 8.4% of them listed that as a major barrier. Inability to access services (5.3%) and language (4.7%) were also reported, especially among non-natives. Interestingly, just 4.5% of respondents claimed that they encountered no obstacles. Furthermore, 9.2% cited other unspecified causes, pointing to other socio-cultural or logistical aspects contributing to the negative attitudes developing premarital screening.
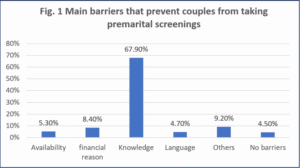
Figure 1: Main barriers that prevent couples from taking premarital screenings
Main barriers that prevent couples’ participants in premarital screening. The chart shows the proportion of respondents indicating different barriers with lack of knowledge as the predominant one (67.9%), other reasons (9.2%), financial reasons (8.4%), availability (5.3%), barriers of language (4.7%), no barriers (4.5%).
The survey results indicate that a majority of participants (87%) recognized the need to enhance public awareness regarding premarital testing and counselling (Figure 2). In contrast, 6.1% believed that existing awareness was sufficient, and 6.3% were uncertain, reflecting a small yet notable gap in public engagement and understanding of the importance of such programs.
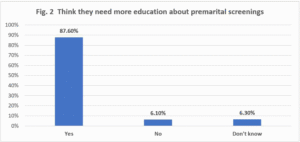
Figure 2: Need for awareness on premarital screenings
Need for knowledge regarding premarital screenings. Most respondents (87.6%) indicated they needed more education, whereas there were a few who indicated no need (6.1%) and not sure (6.3%).
Figure 3 indicates that 28% of the survey participants felt pre-marital screening is useful because it will make family medical history and genetic information readily available in making better and informed marital and reproductive choices. The early identification and management of hereditary conditions was seen by many participants as the main aim of these tests. But a relatively high percentage (15.3%) could not offer more than an incomplete answer, and asked to be given more details, so that although the respondents are aware, their knowledge level with regards to the wider picture of the implications and the advantages of premarital screening is limited amongst some.
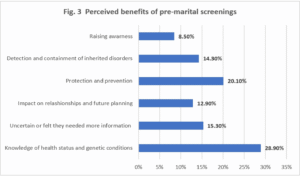
Figure 3. Perceived benefits of pre-marital screenings among participants.
The horizontal bar chart shows respondents’ perceptions of benefits of pre-marital screenings. Health status and genetic conditions (28.9%) as well as protection and prevention (20.1%) were the most frequently cited benefits. The other perceived benefits included necessity for more information (15.3%), detection and containment of inherited disorders (14.3%), effect on relationships and future planning (12.9%) and awareness raising (8.5%).
Discussion
The study assessed the knowledge levels, together with attitudes and practices (KAP), which students in Abu Dhabi, United Arab Emirates demonstrate about premarital screening and consultations. The UAE, along with other countries, prioritize premarital screening as an integral practice because they experience high rates of genetic diseases including thalassemia and sickle cell disease. The study provides crucial insights about the present KAP levels of university students who avoid premarital testing examinations, which lead to productive intervention strategies. When analyzing knowledge scores by marital status, married participants showed significantly greater awareness of screened diseases than their single counterparts. Moreover, postgraduate students exhibited more favorable attitudes toward integrating mental health into premarital screening (92.1%) compared to undergraduates (78.4%), suggesting education level may positively influence screening perceptions. Findings showed premarital health screening knowledge surpasses the evidence of other researchers because of cultural limitations alongside scarce public health programming in different regions [21]. This study also found that a substantial proportion of the respondents (70.8%) were aware of premarital screening and counselling. This level of awareness is relatively high compared to other regions globally, where awareness about premarital health screenings may be lower due to cultural and societal norms or limited public health initiatives [25].
Based on the findings, the most commonly recognized sources of information were family and friends, healthcare workers and media [22]. The study has highlighted the significant role of personal networks and media in the dissemination of health information. However, it can be argued that the impact of education on the families and communities stands equally important to the work of healthcare professionals and media sources in influencing health decisions made by young adults [23, 24]. While media and healthcare professionals play a crucial role, the importance of education within families and communities cannot be overlooked, as it is often the first point of contact for young adults when making decisions about their health [26].
In response to the question concerning genetic diseases, there was a fair knowledge expressed by the respondents on the illnesses which would be widely screened during premarital examinations. In line with the results of Alswaidi et al. [27], the most common responses belonged to the HIV, thalassemia, and hepatitis B diseases, which are common in areas like the UAE. Nonetheless, Syphilis and G6PD deficiency awareness were quite low [28]. These information vacuums are a serious issue, because those who are not aware of such conditions but have advanced to the disorders stage can end up with severe health problems, or even can pass the disorder to their children. Of particular concern is the low awareness level regarding G6PD deficit, an inherited enzyme disorder with a high incidence in the UAE, and can cause serious complications when not detected [29]. Such data reveal that particular educational campaigns targeting the general population and students alike are an extreme necessity. To raise awareness of the informed decision-making process and alleviate the burden of preventable genetic diseases, there is a need to improve knowledge about all conditions that are included in premarital screening.
Most participants supported premarital screening since 85.8% agreed to its effectiveness in minimizing genetic disorder transmission, and 86.1% advocated mandatory premarital testing in the UAE. The findings support positive attitudes about premarital screening, which is aligned with the evidence found by Al-Eissa et al [30], advocating UAE public opinion regarding premarital testing programs. A substantial majority of people supported premarital screening requirements since they view it as fundamental for public health. In the UAE, premarital screenings are identified as a public health policy, making it crucial for citizens. Consistent with these results, studies have also found that people encourage compulsory health tests because these programs deliver clear public health advantages [25, 31].
Although many individuals support premarital screenings, there remains a contrast between awareness and actual engagement with these tests. The majority of participants supported mandatory premarital screenings as beneficial, however, 36.3% of respondents had not undergone premarital screening. Research outcomes revealed differences between student opinions regarding mandatory pre-marital screening and their real-world screening practices. Previous studies argued that public knowledge and positive mindsets toward premarital testing were strong, but actual screening rates remained minimal [15, 32]. It has been found that there are certain barriers to premarital screening implementation, including limited access points and testing costs, as well as cultural opposition to testing procedures. The survey results in the current study showed that 62.4% of respondents had personal connections with couples who skipped premarital screening before their wedding. The study indicates premarital screening has strong community support, but many individuals choose not to follow this recommendation. Research from other countries shows cultural norms affecting premarital screening acceptance rates after identifying negative stigma and discrimination [9, 33]. In societies where discussions on infectious diseases and genetic disorders are deemed culturally inappropriate, they tend to strongly impact premarital screening choices. Individuals in these contexts choose not to have tests for premarital screening because they believe it would expose health conditions to public scrutiny, which would result in family dishonour, leading to stigma and damaging marriage possibilities. Similar to previous research by Zhong et al. [34], cultural norms and concerns about discrimination stop individuals from accessing health services that include premarital screening. The researchers discovered that test-positive individuals experience fear of exclusion from marriage opportunities when their medical results indicate genetic disorders, infectious diseases, or other diseases in cultural environments where health conditions directly affect marital eligibility.
This research examines student behaviours regarding premarital screening practices. Results showed that 64.5% of students said they would reevaluate marriage when their premarital testing detects genetic disorders and compatibility problems. Evidence shows that students not only understand the value of premarital screening but will practice the results to stop genetic diseases from being inherited by the next generation. Research data shows that students who learn about genetic disorder risks make wise decisions for their wedding planning and childbearing [12]. Based on the current findings of this study, 82.7% of respondents supported the inclusion of mental health screenings in premarital examinations. Emerging evidence shows that society increasingly understands that mental health needs recognition in the comprehensive understanding of personal well-being, specifically within marriage.
Studies favor the inductance of psychiatric assessments into premarriage screening projects since the psychological health is a great contributing factor to marital happiness and long-term relationship stability [35]. Depression, anxiety, and personality disorders have been found to affect marital dynamics negatively; pre-marriage assessments can reduce these risks by identifying them early [36, 37]. Mental health should also be added to the screening procedures, as it will help eliminate the stigma around mental problems, prompting individuals to address them in time [38, 39]. Such concurs with the findings of the present study, as two-thirds of the participants were open to recommending screening of a future spouse, particularly males (85.7%) and females (70.0%). These findings indicate an increasement in the awareness of preventative health in the youth. Moreover, students in young adults who are inbuilt to social and academic networks can become instrumental in information diffusion. University students may respond well to a public health campaign that aims to raise awareness, advance positive attitudes, and involvement in premarital screening services.
The current study found multiple obstacles preventing people from accessing premarital testing, although public attitudes basically accepted this practice. Financial challenges emerged as the main blocking factor during the study, and language barriers, together with service availability issues, followed in the second position. The percentage of people reporting financial constraints stood at 8.4%, but the figures could indicate barriers for specific population groups with lower incomes. The government of the UAE ensures citizens have health insurance that provides medical coverage, clearing financial obstacles from their path, unlike many other regions in the world [40]. Costly premarital screening creates an insurmountable financial burden for those without government insurance or UAE citizenship. The availability of premarital screening services and language differences caused barriers that prevented 5.3% and 4.7% of patients from obtaining necessary tests before marriage. The implementation of better language support with distributed service networks can improve premarital screening accessibility. A wide range of language options combined with sufficient medical services in both city and country locations of the UAE would improve premarital testing uptake rates. The research delivers important findings about how Abu Dhabi University students perceive and execute premarital screening programs. Premarital screening programs that incorporate mental health evaluation with peer-support programs to prevent genetic disorders will enhance public health results [41]. The understanding of how precise health education methods affect premarital screening recognition rates, together with their ability to remove barriers, should receive additional study application in the population of the United Arab Emirates.
Conclusion
This research evaluated student perceptions about premarital testing operations in Abu Dhabi, UAE, through their knowledge, attitudes, and practical understandings (KAP). Data showed that students were highly informed about premarital screening because 70.8% of them knew what it meant. The results showed that students from Abu Dhabi strongly accepted making premarital testing mandatory in the UAE, with 85.8% agreement about its importance to limit genetic disease transmission and 86.1% support for this policy. The study demonstrated positive attitudes among participants and high levels of awareness, yet discovered important implementation gaps.
The research findings showed that students possessed strong awareness and positive views, but highlighted various weaknesses in premarital screening practices. According to survey results, 36.3% of respondents admitted to receiving premarital testing. Students seem to understand why premarital screening matters, but their participation in the screening process remains inconsistent. The study revealed vital obstacles to participation in premarital screening services, which must be resolved to increase service utilization. Lack of premarital screening resulted in many study subjects knowing people who underwent weddings without necessary examinations, leading to educational initiatives to show the value of these screenings. Based on the study findings, 82.7% of participants endorsed mental health assessment for premarital screening as an essential component of the process. Society has demonstrated increased understanding about mental health’s vital influence on marriage, which implies adding mental health assessments will boost the success of premarital screening programs.
Health initiatives and public education programs should be implemented to raise awareness about all premarital screening tests, especially rare diseases with low awareness, such as G6PD deficiency and syphilis. For higher participation rates, we must overcome both financial obstacles and language-related obstacles to accessing these services. The achievement of healthcare equity requires the provision of multilingual services along with affordable screening access for non-citizens. Mental health screenings incorporated within premarital checks would enhance global understanding about how mental state conditions extend marital durations. However, multiple factors limit the conclusions drawn from this research, although it yields significant knowledge. University students at Abu Dhabi University might not represent all population demographics of the United Arab Emirates. A comprehensive examination of non-participants in premarital testing was insufficient in this research so additional qualitative approaches should be pursued to determine their motivations.
Declarations
Ethical Approval: All procedures in this study were based on the guidelines in the 2013 version of the Declaration of Helsinki. Research tasks carried out with human volunteers were done according to the ethical guidelines decided by the research committees. Human participants agreed to participate only when they had given informed consent. Ethical standards were applied throughout this study as per Dubai Health Authority guidelines and regulations. Ethical approval was obtained from the Abu Dhabi University IRB committee under Approval Certificate number CHS-000001.
Informed Consent Statement: Informed consent was obtained from all subjects involved in the study.
Data Availability Statement: The datasets generated and analyzed during the current study are not publicly available because the data analysis is ongoing to study variables other than those covered in this study but are available from the corresponding author and with permission of the Abu Dhabi University on reasonable request.
Competing Interest: The authors declare that they have no competing interests.
Funding: This research received no external funding.
Contributors:
R.K., guided the research through his role as undergraduate research advisor while helping with ideas and methods and inspecting the final manuscript. All authors including K.M.K.A., A.M.O., A.M.A. and O.A.S. made equal contributions throughout the research by collecting data and analyzing it while interpreting results and writing the manuscript and providing vital intellectual revisions. The guarantor of the study, K.M.K.A., is responsible for maintaining the research’s integrity throughout the study and its findings. H.M critically reviewed the manuscript.
Acknowledgements: The authors express gratitude toward Abu Dhabi University together with the Health Sciences College within the Department of Public Health for their continuous support of this research. They give particular appreciation to the Institutional Review Board, which provided both ethical authorization and research process support. We profoundly thank each student who volunteered for the study since their contributions helped generate essential knowledge for our research. These students made it possible to gain essential insights into premarital screening practices in the UAE by participating in the study.
References
[1].Hu JX, Nash ST. Marriage and the family: Mirror of a diverse Global Society.
Routledge; 2019 Apr 23.
[2].Al-Krenawi A, Jackson SO. Arab American marriage: Culture, tradition, religion, and the social worker. Journal of Human Behavior in the Social Environment. 2014 Feb 17;24(2):115-37.
[3].Rahman MM, Naznin L, Giti S, Islam MS, Khatun N. Premarital health screening a review and update. Journal of Armed Forces Medical College, Bangladesh. 2014;10(1):103-9.
[4].Kooli C, Abadli R. The relevance and impact of laws regulating premarital screenings in the Muslim Arab countries. Journal of Sharia and Islamic Studies. 2018;35(120):281- 332.
[5].Tadmouri GO. Genetic disorders. InCaring for Arab Patients 2018 Dec 20 (pp. 61-74).
CRC Press.
[6].Bener A, Abdulrazzaq YM, Al-Gazali LI, Micallef R, Al-Khayat AI, Gaber T. Consanguinity and associated socio-demographic factors in the United Arab Emirates. Human heredity. 1996 Sep 3;46(5):256-64.
[7].MoHAP. Genetic testing as part of premarital screening for Emiratis [Internet]. Ministry of Health and Prevention – UAE. 2023 [cited 2025 May 5]. Available from: https://mohap.gov.ae/en/w/genetic-testing-as-part-of-premarital-screening-for- emiratis
[8].ROSHAN BS. Prevalence of At-Risk Marriages among Couples Attending Premarital Screening (PMS) Programs: A Systematic Review and Meta-Analysis.
[9].Al-Shafai M, Al-Romaihi A, Al-Hajri N, Islam N, Adawi K. Knowledge and perception of and attitude toward a premarital screening program in Qatar: a cross-sectional study. International journal of environmental research and public health. 2022 Apr 6;19(7):4418.
[10]. Jameel T, Baig M, Murad MA, Gazzaz ZJ, Mal Y, Alyoubi WE, Alyoubi GH, Alaslani ST, Alshuaibi HA, Nawaz A, Alkaabi T. Consanguineous marriages, premarital screening, and genetic testing: a survey among Saudi university students. Frontiers in Public Health. 2024 Mar 21;12:1328300.
[11]. Al Kindi R, Al Rujaibi S, Al Kendi M. Knowledge and attitude of university students towards premarital screening program. Oman medical journal. 2012 Jul;27(4):291.
[12]. Melaibari M, Shilbayeh S, Kabli A. University students’ knowledge, attitudes, and practices towards the national premarital screening program of Saudi Arabia. Journal of Egyptian Public Health Association. 2017 Mar 1;92(1):36-43.Alkhaldi SM, Khatatbeh MM, Berggren VE, Taha HA. Knowledge and attitudes toward mandatory premarital screening among university students in North Jordan. Hemoglobin. 2016 Mar 3;40(2):118-24.
[13]. Alwhaibi RM, Almuwais AK, Alotaibi M, AlTaleb HM, Alsamiri SM, Khan R. Health beliefs of unmarried adult Saudi individuals toward safe marriage and the role of premarital screening in avoiding consanguinity: a nationwide cross-sectional study. Frontiers in Public Health. 2024 Jun 19; 12:1379326.
[14]. Al-Farsi OA, Al-Farsi YM, Gupta I, Ouhtit A, Al-Farsi KS, Al-Adawi S. A study on knowledge, attitude, and practice towards premarital carrier screening among adults attending primary healthcare centers in a region in Oman. BMC Public Health. 2014 Dec; 14:1-7.
[15]. Van Buren F, Van Gordon W. Emirati women’s experiences of consanguineous marriage: a qualitative exploration of attitudes, health challenges, and coping styles. International Journal of Mental Health and Addiction. 2020 Aug;18(4):1113-27.
[16]. Simkus J. Snowball sampling method: Techniques & examples. Simply Psychology.[Veebileht] Https://Www. Simplypsychology. Org/Snowball-Sampling. Html (20.05. 2024). 2023.
[17]. Adeoye MA. Review of sampling techniques for education. ASEAN Journal for Science Education. 2023;2(2):87-94.
[18]. Srinivasan R, Lohith CP, Srinivasan R, Lohith CP. Pilot Study—Assessment of validity and reliability. Strategic marketing and innovation for Indian MSMEs. 2017:43-9.
[19]. Bala J. Contribution of SPSS in Social Sciences Research. International Journal of Advanced Research in Computer Science. 2016 Nov 1;7(6).
[20]. Al Eissa MM, Almsned F, Alkharji RR, Aldossary YM, AlQurashi R, Hawsa EA, AlDosari SM, Alqahtani AS, Alotibi RS, Farzan R, Alduaiji R. The perception of genetic diseases and premarital screening tests in the central region of Saudi Arabia. BMC Public Health. 2024 Jun 10;24(1):1556.
[21]. Eysenbach G. Credibility of health information and digital media: New perspectives and implications for youth. 2007 Aug 12.
[22]. Wallack LM. Media advocacy and public health: Power for prevention. sage; 1993 Oct 7.
[23]. National Academies of Sciences, Medicine, Board on Global Health, Committee on Educating Health Professionals to Address the Social Determinants of Health. A framework for educating health professionals to address the social determinants of health.
[24]. Rahman MM, Naznin L, Giti S, Islam MS, Khatun N. Premarital health screening a review and update. Journal of Armed Forces Medical College, Bangladesh. 2014;10(1):103-9.
[25]. Watson D, Mhlaba M, Molelekeng G, Chauke TA, Simao SC, Jenner S, Ware LJ, Barker M. How do we best engage young people in decision-making about their health? A scoping review of deliberative priority setting methods. International Journal for Equity in Health. 2023 Jan 25;22(1):17.
[26]. Alswaidi FM, O’brien SJ. Premarital screening programmes for haemoglobinopathies, HIV and hepatitis viruses: review and factors affecting their success. Journal of medical screening. 2009 Mar;16(1):22-8.
[27]. Mithila SN. A Study on Knowledge, Perception and Attitude Towards Premarital Carrier Screening (PMCS) Among Students Attending Universities (Doctoral dissertation, East West University).
[28]. Alangari AS, El-Metwally AA, Alanazi A, Al Khateeb BF, Al Kadri HM, Alshdoukhi IF, Aldubikhi AI, Alruwaili M, Alshahrani A. Epidemiology of glucose-6-phosphate dehydrogenase deficiency in Arab countries: Insights from a systematic review. Journal of Clinical Medicine. 2023 Oct 20;12(20):6648.
[29]. Al Eissa MM, Almsned F, Alkharji RR, Aldossary YM, AlQurashi R, Hawsa EA, AlDosari SM, Alqahtani AS, Alotibi RS, Farzan R, Alduaiji R. The perception of genetic diseases and premarital screening tests in the central region of Saudi Arabia. BMC Public Health. 2024 Jun 10;24(1):1556.
[30]. Miles A, Cockburn J, Smith RA, Wardle J. A perspective from countries using organized screening programs. Cancer: Interdisciplinary International Journal of the American Cancer Society. 2004 Sep 1;101(S5):1201-13.
[31]. Mahmood KA, Sadraldeen GS, Othman SM, Shabila NP, Saleh AM, Ismail KH. Knowledge, perception, and attitude toward premarital screening among university students in Kurdistan region–Iraq. PLOS Global Public Health. 2024 Nov 18;4(11):e0003515.
[32]. Alkalbani A, Alharrasi M, Achura S, Al Badi A, Al Rumhi A, Alqassabi K, Almamari R, Alomari O. Factors Affecting the willingness to undertake premarital screening test among prospective marital individuals. SAGE open nursing. 2022 Feb;8:23779608221078156.
[33]. Zhong A, Darren B, Loiseau B, He LQ, Chang T, Hill J, Dimaras H. Ethical, social, and cultural issues related to clinical genetic testing and counseling in low-and middle- income countries: a systematic review. Genetics in Medicine. 2021 Dec;23(12):2270- 80.
[34]. Shahhosseini Z, Hamzehgardeshi Z, Kardan-Souraki M. The effects of premarital relationship enrichment programs on marriage strength: A narrative review article. Journal of Nursing and Midwifery Sciences. 2014 Oct 10;1(3):62-72.
[35]. Joseph D. The effectiveness of premarital counseling assessments on marital satisfaction. Argosy University, Tampa; 2014.
[36]. Halford WK, Markman HJ, Kling GH, Stanley SM. Best practice in couple relationship education. Journal of marital and family therapy. 2003 Jul;29(3):385-406.
[37]. Corrigan PW, Druss BG, Perlick DA. The impact of mental illness stigma on seeking and participating in mental health care. Psychological science in the public interest. 2014 Oct;15(2):37-70.
[38]. Crowe A, Averett P, Glass JS. Mental illness stigma, psychological resilience, and help seeking: What are the relationships?. Mental Health & Prevention. 2016 Jun 1;4(2):63- 8.
[39]. Koornneef E, Robben P, Blair I. Progress and outcomes of health systems reform in the United Arab Emirates: a systematic review. BMC health services research. 2017 Dec;17:1-3.
[40]. Essien EA, Winter-Eteng BF, Onukogu CU, Nkangha DD, Daniel FM. Psychosocial challenges of persons with sickle cell anemia: A narrative review. Medicine. 2023 Nov 24;102(47):e36147.
Table 1: Sociodemographic characteristics of the participants
| Characteristic | Frequency (N) | Percentage (%) |
| Age | ||
| 18-28 | 273 | 71.8% |
| 29-39 | 74 | 19.5% |
| 40-50 | 25 | 6.6% |
| 51-60 | 8 | 2.1% |
| Gender | ||
| Female | 280 | 73.7% |
| Male | 100 | 26.3% |
| Citizenship | ||
| UAE citizen | 179 | 47.1% |
| All other nationalities | 201 | 52.9% |
| Marital Status | ||
| Single | 256 | 67.4% |
| Married | 88 | 23.2% |
| Divorced | 11 | 2.9% |
| Separated | 16 | 4.2% |
| Widowed | 9 | 2.4% |
| Educational Attainment | ||
| High School/Diploma | 137 | 36.1% |
| Bachelor’s Degree | 186 | 48.9% |
| Postgraduate Degree | 57 | 15.0% |
| Employment Status | ||
| Employed | 158 | 41.6% |
| Unemployed | 222 | 58.4% |
| Income | ||
| Under 5,000 AED | 176 | 46.3% |
| 5,000 – 20,000 AED | 135 | 35.5% |
| Over 20,000 AED | 69 | 18.2% |
Table 2: Participants’ knowledge about pre-marital screenings and counselling
| Item | Frequency (N) | Percentage (%) |
| Heard of premarital screenings and counselling | ||
| Yes | 269 | 70.8% |
| No | 68 | 17.9% |
| I don’t know | 43 | 11.3% |
| Source of knowledge | ||
| Family | 118 | 31.1% |
| Friends | 40 | 10.5% |
| Healthcare workers | 84 | 22.1% |
| Media | 60 | 15.8% |
| University | 29 | 7.6% |
| I have never heard about it | 49 | 12.9% |
| Heard of the following diseases | ||
| HIV | 214 | 56.3% |
| Thalassemia | 195 | 51.3% |
| Hepatitis B | 183 | 48.2% |
| Sickle cell disease | 153 | 40.3% |
| G6PD | 76 | 20.0% |
| Syphilis | 104 | 27.4% |
| I don’t know any of them | 55 | 14.5% |
| Knew that PMCS reduces the spread of hereditary diseases | ||
| Yes | 326 | 85.8% |
| No | 13 | 3.4% |
| I don’t know | 41 | 10.8% |
| Premarital screening is mandatory in the UAE | ||
| Yes | 327 | 86.1% |
| No | 14 | 3.7% |
| I don’t know | 39 | 10.3% |
| Neglecting premarital screening may affect the relationship | ||
| Yes | 303 | 79.7% |
| No | 31 | 8.2% |
| I don’t know | 46 | 12.1% |
| Premarital screening could reduce the chance of psychological or social issues | ||
| Agree | 326 | 85.8% |
| Disagree | 15 | 3.9% |
| I don’t know | 39 | 10.3% |
| Knowing someone who married without screening | ||
| Yes | 237 | 62.4% |
| No | 143 | 37.6% |